Anatomy and Physiology Pearls
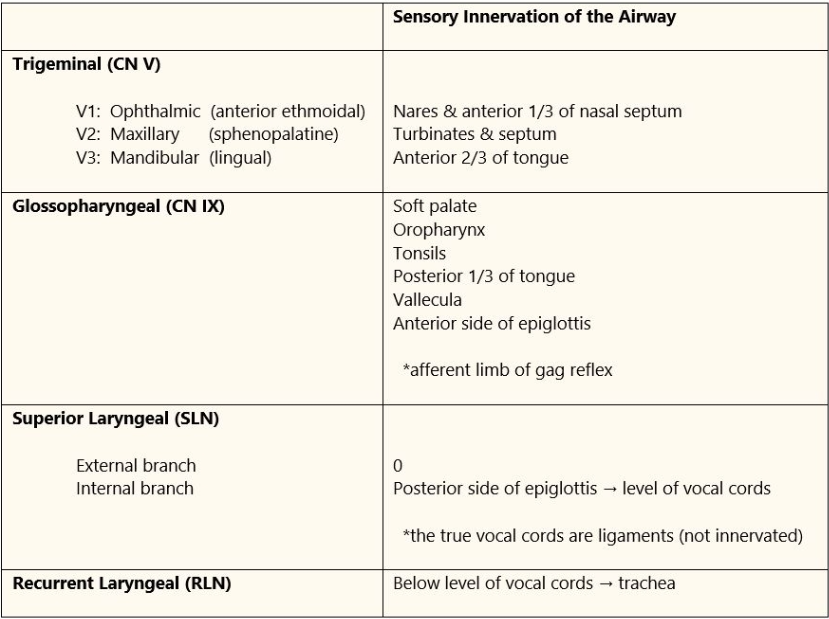
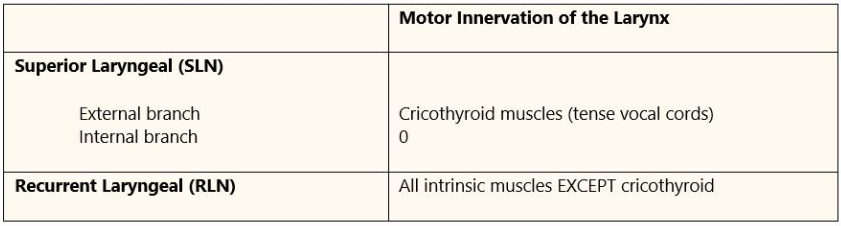
Airway Innervation
Alpha 1 Antitrypsin Deficiency
- Made in liver and stops enzyme alveolar elastase
- Deficiency causes destruction of pulmonary connective tissue resulting in panlobular emphysema
Anticholinergic / Cholinergic Syndromes
Anticholinergic
- Antimuscarinic use (scopolamine)
- Minimal temp inc, dry mouth, delirium, dry skin, midriasis
- Tx: Physostigmine (only one that can cross BBB)
Cholinergic
- Organophosphates, nerve agents, nicotine poisoning, cholinesterase inhibitor OD (myasthenia pts)
- Tx: Antimuscarininc drugs such as atropine, if resp compromise intubate and wait for acetylcholine level to come down (no way to reverse nicotinic receptor issue)
Autonomic Hyperreflexia
- Stimulation of sympathetic nervous system below level of spinal cord injury (bladder catheter etc)
- Causes HTN emergency due to lack of inhibitory reflexes below injury and bradycardia
- Tx: Deepen anesthetic or use rapid acting vasodilators
- GA and spinal best anesthetic choice
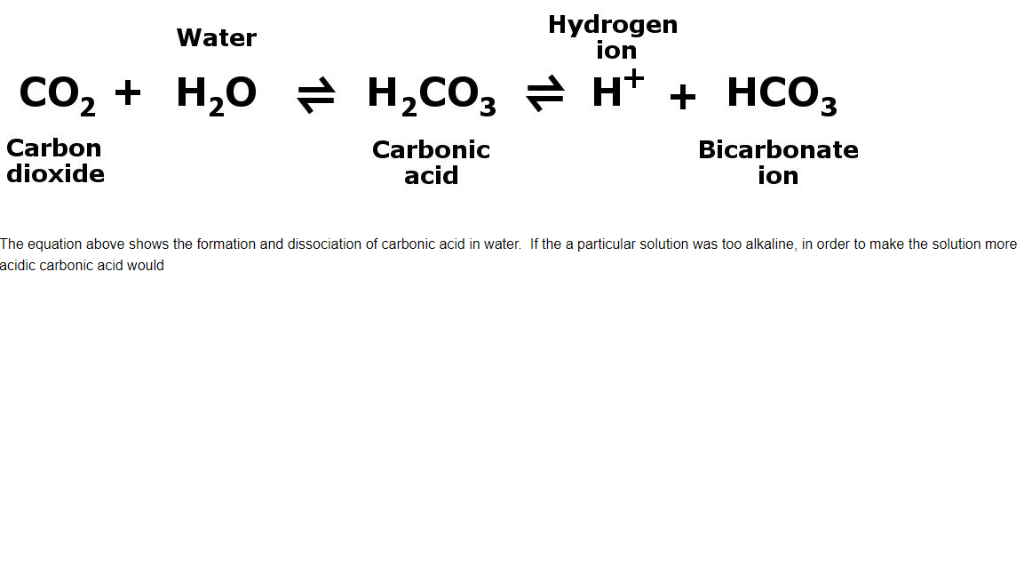
Bicarbonate
- Hyperosmolar, hypervolemia, hypernatremia, together cause inc ICP
- Left shift from bicarb on oxyhgb curve lasts up to 8 hrs dec PaO2
- Dec ionized calcium
- Need to replace calcium with bicarb admin
Administer Bicarbonate only in nongap acidosis such as renal tube acidosis, hyperk, diarrhea, enterocutaneous fistula. Consider bicarb in lactic acidosis if ph< 7.1 Minimal research to back this up. Rta type 1 is related to Ehler danlos, uti, sickle. RTA type 2 with rickets. RTA type 4 seen with urinary obstruction, immunosuppressants, kidney rejection. Also seen with many meds like diuretics and ace. Symptoms are high potassium and low bicarb.
- Probably not beneficial in cardiac surgery
- Bicarb is not shown to dec PVR, improve response to pressors, or inc CO
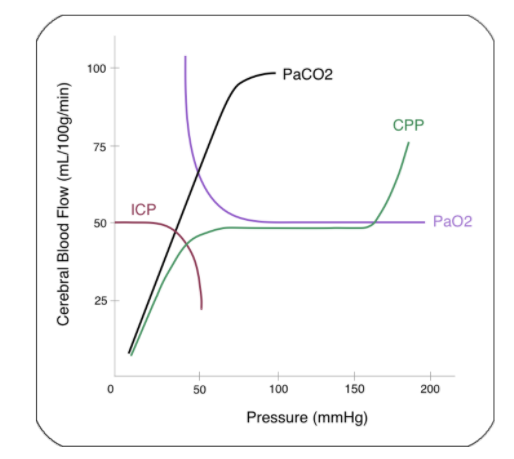
Cerebral Blood Flow
CO2 Curve
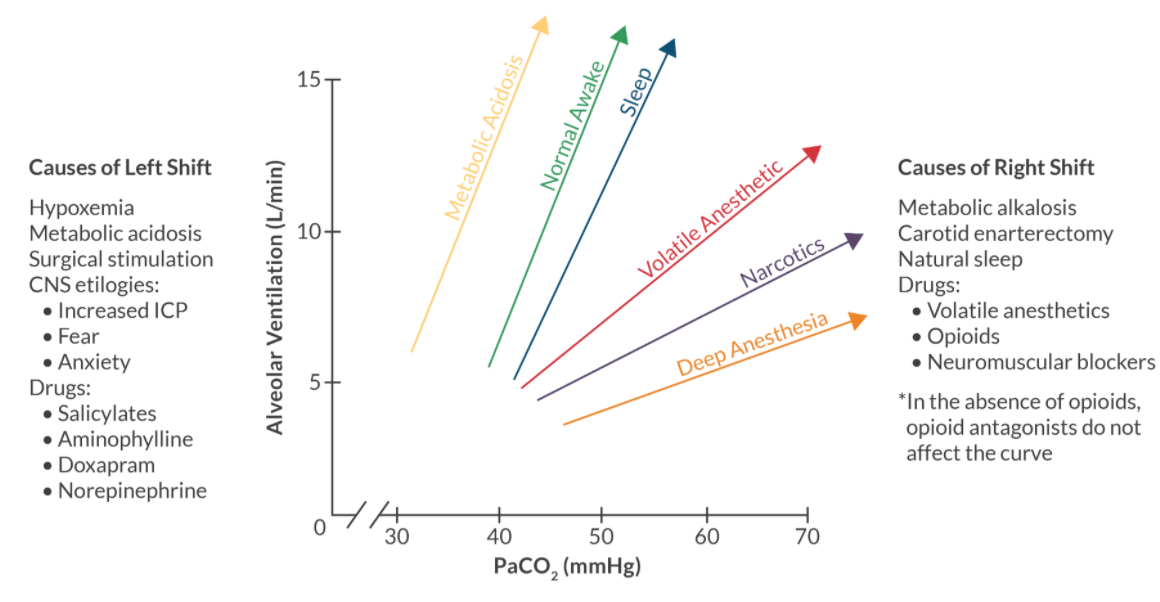
Bohr Effect
- CO2 and decreased pH cause erythrocytes to release O2
Haldane Effect
- O2 causes the erythrocyte to release CO2
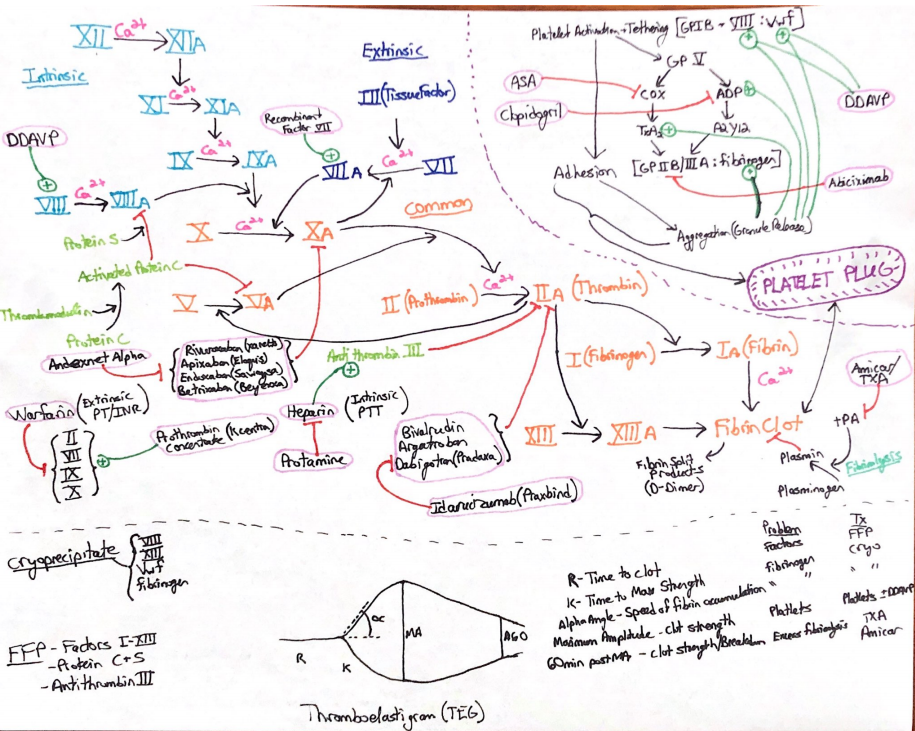
Coagulation Cascade
Electrolye Review
Calcium
- Parathyroid Hormone
- Inc Ca release from bones (osteoclast)
- Inc renal reabsorption
- Inc Vit D3 activation (VitD comes from skin and is made into D3 in liver and activated in kidney)
- Inc Ca reabsorption in intestines
- Calcitonin
- Dec Ca release from bones
- Bisphosphonates
- Treatment for hypercalcemia
- Secondary hyperPTH
- Caused by decreased kidney function and or decreased Vit D3
Potassium
- Shift into Cell:
- Insulin (Na/K/ATPase)
- Aldosterone (Conn syndrome causes hypokalemia)
- Beta Agonist
- Alkalosis
- Shift Out
- Dec Insulin (DM)
- Addisons (Dec aldosterone)
- Beta Blockade
- Acidosis (Dec fx of Na/K/ATPase)
- Exercise (cell lysis)
Heart Failure Review
Diastolic
- Preserved EF
- Pressure work
- Hypertrophy
- Want nl preload, nsr, and dec afterload to help dec tissue remodel
- Give beta and calcium channel blockers
- Norepi for pressor
Systolic
- Dec EF
- Volume work
- Dilated
- Want nl preload, nsr, and dec afterload due to weak ventricle
- Give inotropes and vasodilators
High Altitude Physiology Review
- Cerebral edema: hypoxia and vascular dilation
Pulmonary edema: hypoxia causes vasoconstriction which inc capillary pressure: right heart failure eventually
- Tx with Acetazolamide to acidify the blood and inc ventilation (Carbonic anhydrase inhibitor)
- Nifedipine to stop vasoconstriction in lungs
Neuroleptic Malignant Syndrome
- Dopamine Antagonist (1-3 days)
- Very inc temp, drooling, palor, coma, dec reflex, unstable autonomic nervous system (inc/dec BP/HR)
- Tx: Stop dopamine antagonist, give dopamine agonist (Bromocriptine, amantadine), IV fluid, cooling, benzos for agitation, Dantrolene for muscle relaxation
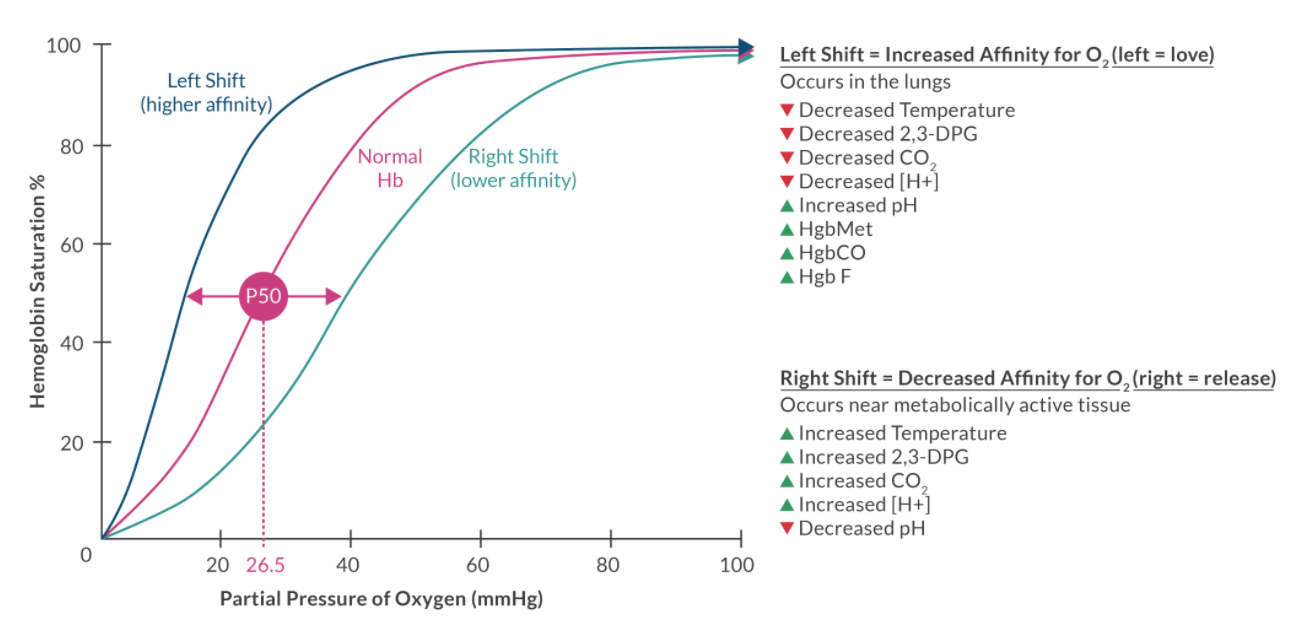
Oxyhemoglobin Dissociation Curve
Pain
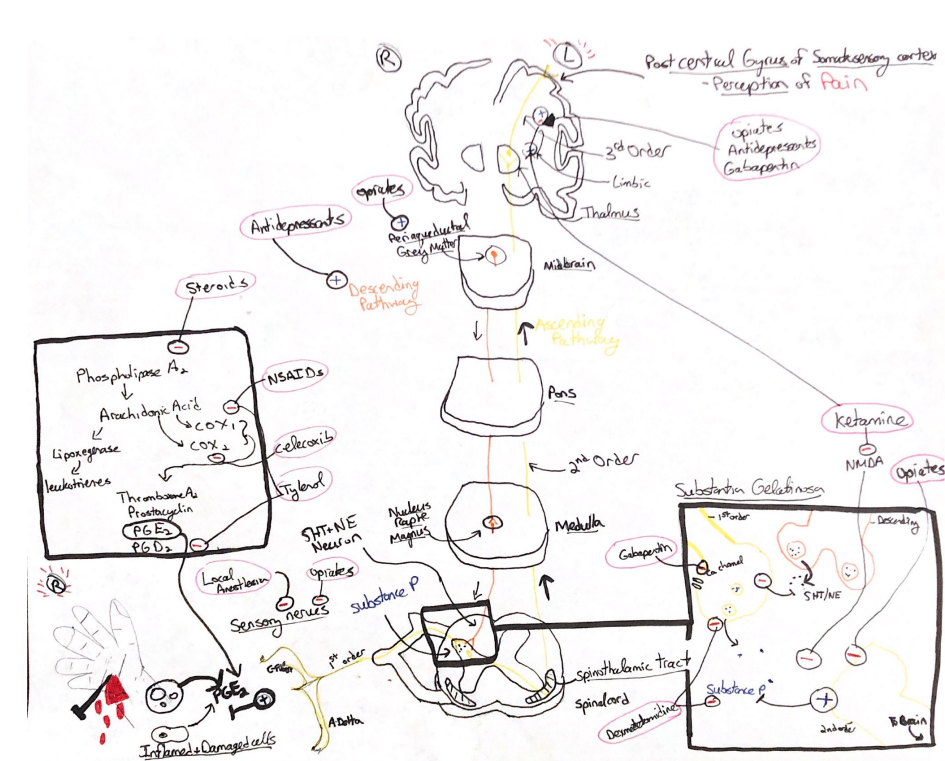
Pain Pathway
- Tranduction: injury causes activation of fast A-Delta and slow C fibers. Substance P is released
- Target Drugs: Local Anesthetic Cream, NSAIDs, Opioids
- Transmission: Signals travel towards the brain via the spinothalamic tract
- Target Drugs: Local Anesthetic blockade
- Modulation: Within the substantia gelatinosa of the spinal cord
- Inhibition via the descending inhibitory pathway: 5HT and NE, effect inc with antidepressants
- Augmentation via central sensitization and wind up: Blocked by ketamine and precedex
- Secondary Hyperalgesia: Inc substance P, triple response of dilation, erythema, wheal
- Primary Hyperalgesia: PGE2 stimulates free nerve endings
- NSAIDs and Steroids block PGE2
- Tylenol may antagonise cannabinoid receptors or a possible COX 3 - Target Drugs: NMDA anatagonists, Neruaxial Opioids, Alpha-2 Agonists, SNRIs
- Perception
- Target Drugs: General Anesthetics, Opioids, Alpha-2 Agonists
Opiates
- Mu1: classic opiate effects
- Mu2 dependence, spinal analgesia
- Mu3 Immunosuppression
- Kappa: Dysphoria, hallucination, Antishiver
- Delta: Itching
Renal Review
AKI
- Prerenal :
- Dec blood flow/oxygen d/t dec volume
- Burns
- Vomit
- Sepsis
- Renal artery stenosis/thrombosis
- Intrarenal :
- Glomerulonephritis
- HTN
- Pylo
- Acute Tubular Necrosis (ischemic, or medication/toxin)
- Post Renal
- Stones/obstruction
CKD
List of signs/symptoms:
Uremia, azotemia (inc nitrogen), edema, ascites, anemia (d/t dec erythropoietin), osteomalacia (dec vit D activation and inc phosphate retention)
Nephrotic Syndrome
- Loss of proteins across kidney tubules: from chronic glomerulonephritis, amyloidosis
- Causes dec osmotic pressure and profound edema
Respiratory Tests/Spirometry
Closing Volume
- Volume at which dynamic airway compression occurs
- Inc with age, obstructive disease, obesity, preggo
Closing Capacity
- Closing Volume + Residual Volume
- Normally in spontaneously ventilating pts FRC > CC so airways do not collapse
- If FRC < CC airways collapse during normal tidal breathing leading to dec O2 sat, inc shunt
- Tx with peep
Residual Volume
- Not measured in spirometry
- Increased in obstructive disease
- Decreased in restrictive disease
Total Lung Capacity
- Increased or normal in obstructive disease
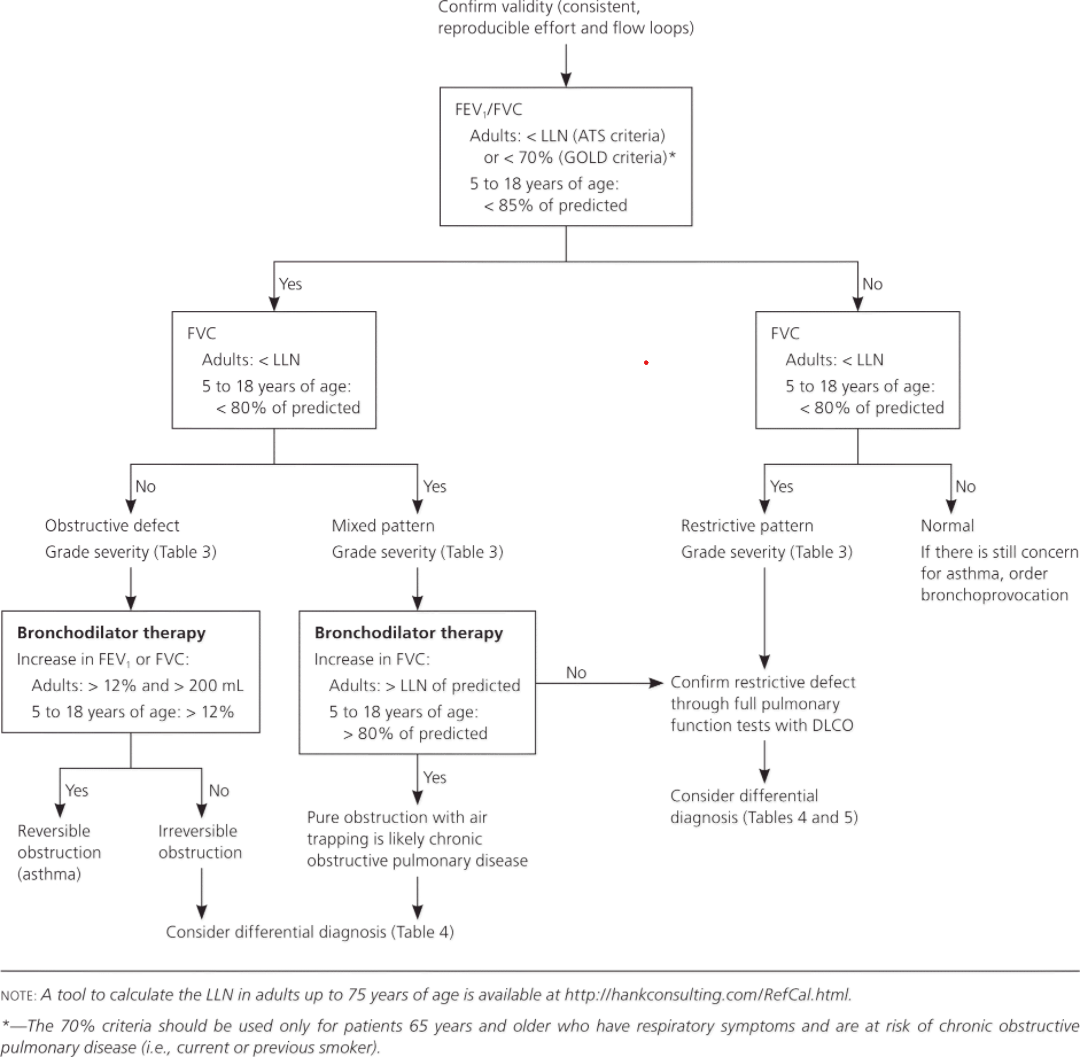
Interpreting PFTs
Serotonin Syndrome
Signs/Symptoms
- Inc temp, inc reflex, drooling, coma, agitated, sweating
Causes
- SSRI/SNRI especially with MAOI
- Inc risk with: linezolid, methylene blue, lithium, fentanyl, stimulants like amphetamine, cipro, Erythromycin
Treatment
- Cooling, IV fluids, paralysis/vent if temp uncontrolled 41C<, cyproheptadine, benzos
Thyroid Review
- TRH – TSH – T4 – T3 (activated T4-T3 in cells)
- Levothyroxine (T4)
- Hyperthyroid Tx: Methimazole, Propylthiouracil (stops T4-T3), No amiodarone due Iodine
- Thyroid Storm: Propranolol is best beta blocker (stops T4-T3) and PTU
This post is licensed under CC BY 4.0 by the author.