Vasoplegia in Cardiac Surgery
Vasoplegia
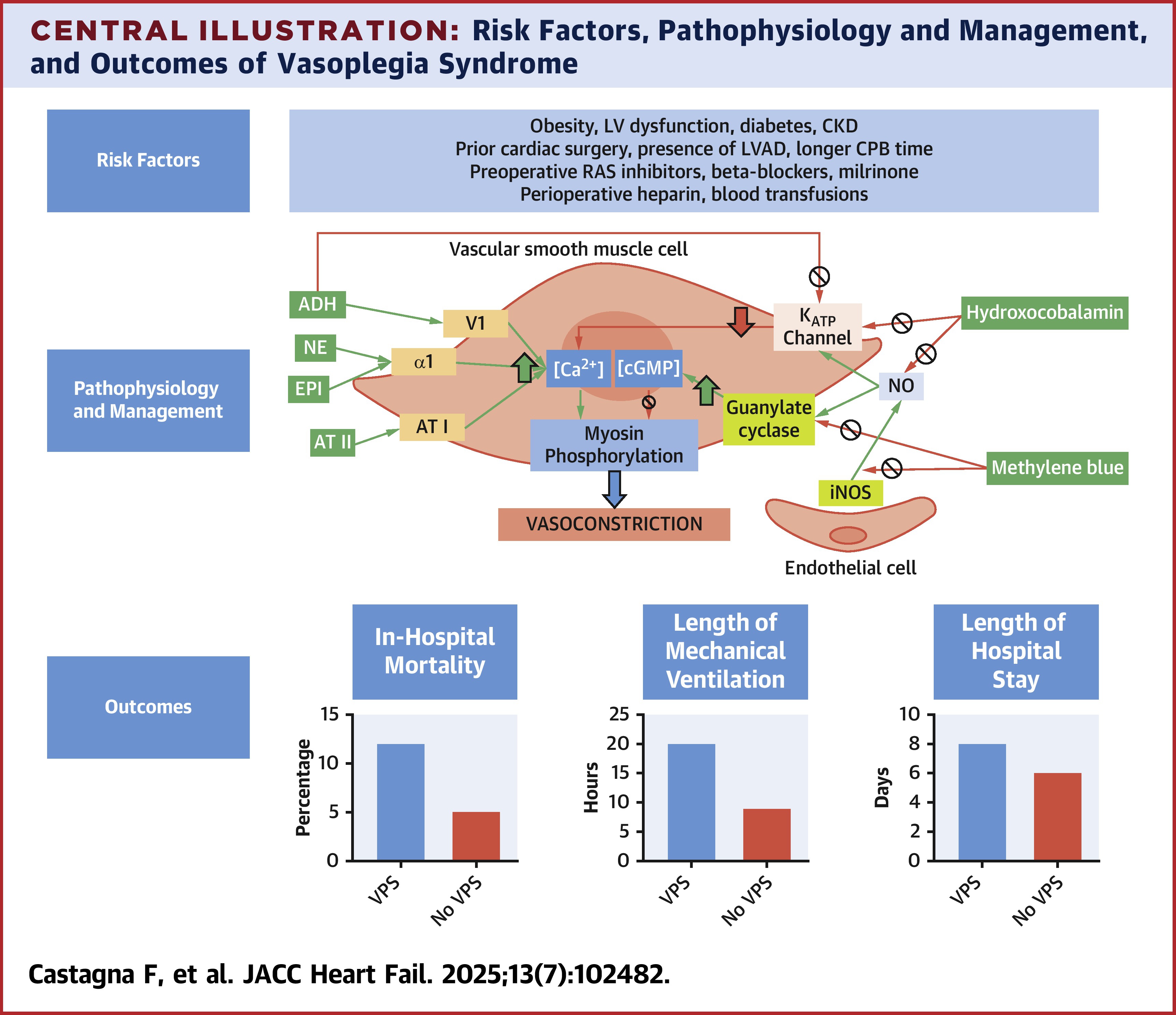
Vasoplegia is a type fo distributive shock that follows cardiac surgery in up to 25% of cases. This leads to prolonged ICU stays, renal fialure, and increased mortality. Catecholamine resistant vasoplegia can be lethal with mortality rates approaching 25%. Vasoplegia can also exist in septic shock, end stage liver disease, and glucocorticoid deficiency.
Risk Factors
- Preoperative ACEi
- Higher comorbid disease burden
- Low preop EF
- Vasopressor support before and/or during CPB
- Warmer core temperature on CPB
- Long cross clamp time
Criteria
- MAP < 65 with an index of > 2.2
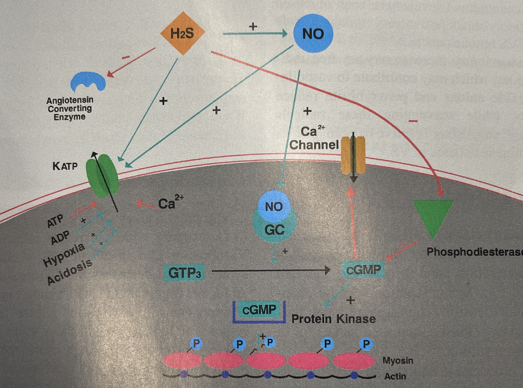
Physiology Simplified
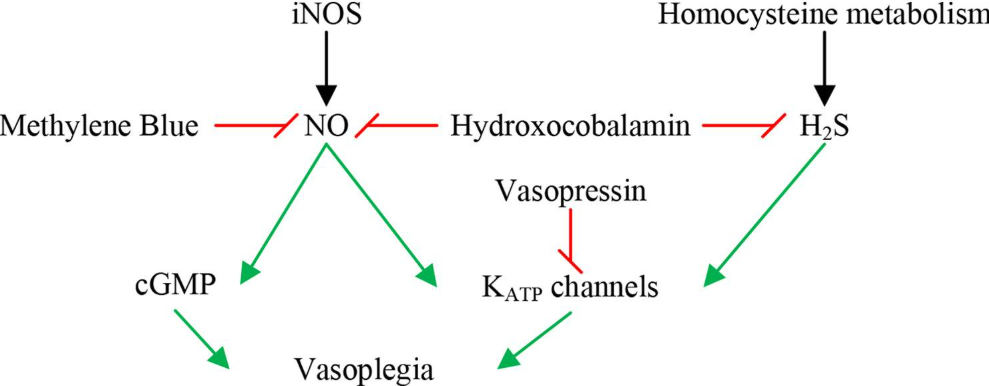
Specific Effect of H2S and NO
Treatment Goals
- Restore and Maintain MAP
- Vasopressors
- Inhibit vasodilatory mediators
- Methylene blue vs Hydroxocobalamin
- Goal directed fluid admin
- Improve Tissue Perfusion
- Fluids
- Inotropes
- Mechanical Support
- Prevent End Organ Damage
- Anemia treatment
- Assess renal, respiratory and cardiac function
- Identify and Treat Causes
- Immune suppression
- Steroids
- Histamine blockers
- Ascorbic acid/Thiamine
- Assess other factors
- Acidosis
- Hypovolemia
- Cardiogenic Shock
- Sepsis
- Medication/Transfusion Reaction
- Anaphylaxis
- Adrenal/Thyroid Crisis
- Immune suppression
Treatment Regimen
This is in order for the most part. I would recommend angiotensin II or vaso before epinephrine if the cardiac function is okay.
- Norepinephrine (0.02-0.5mcg/kg/min)
- Vasopressin (0.02-0.1un/min)
- Epinephrine (0.01-0.2mcg/kg/min)
- Angiotensin II (5-40ng/kg/min)
- Methylene Blue (1-2mg/kg bolus in 15min +/- 0.5-1mg/kg/hr infusion)
- Hydroxocobalamin (5g bolus over 15min can repeat x1)
- Hydrocortisone (50mg q6h or 100mg q8hr)
- Ascorbic acid (6g daily in divided doses per pharmacy)
- Thiamine (400 mg daily)
- Diphenhydramine (25-50mg q4-6h max 400mg in 24hr)
Comparison Between Methylene Blue and Hydroxocobalamin
A small sample size study showed no difference between the two treatment options when faced with vasoplegia status post cardiac bypass.
Summary
This post is licensed under CC BY 4.0 by the author.