Mechanical Support
ECMO Circuit Review¶
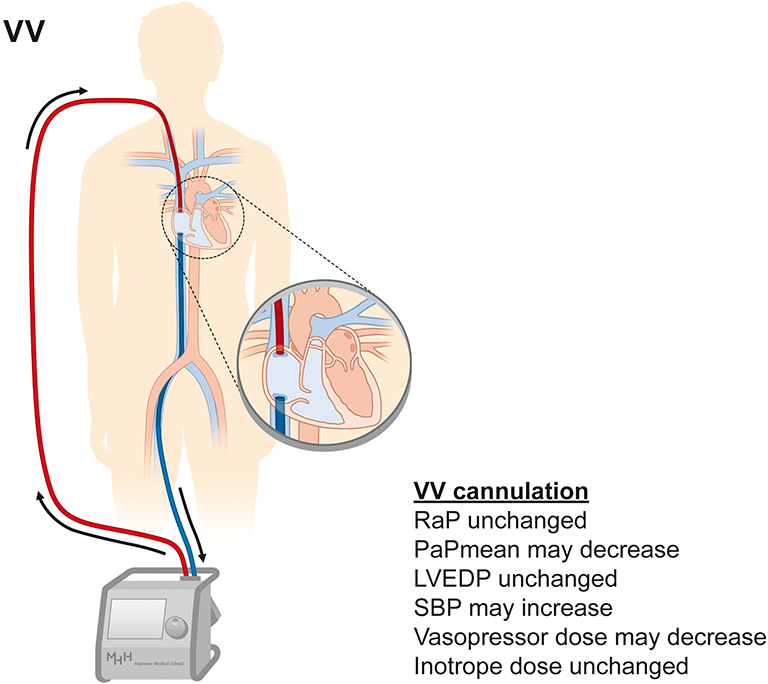
VV ECMO¶
Most common for lung issues such as ARDS
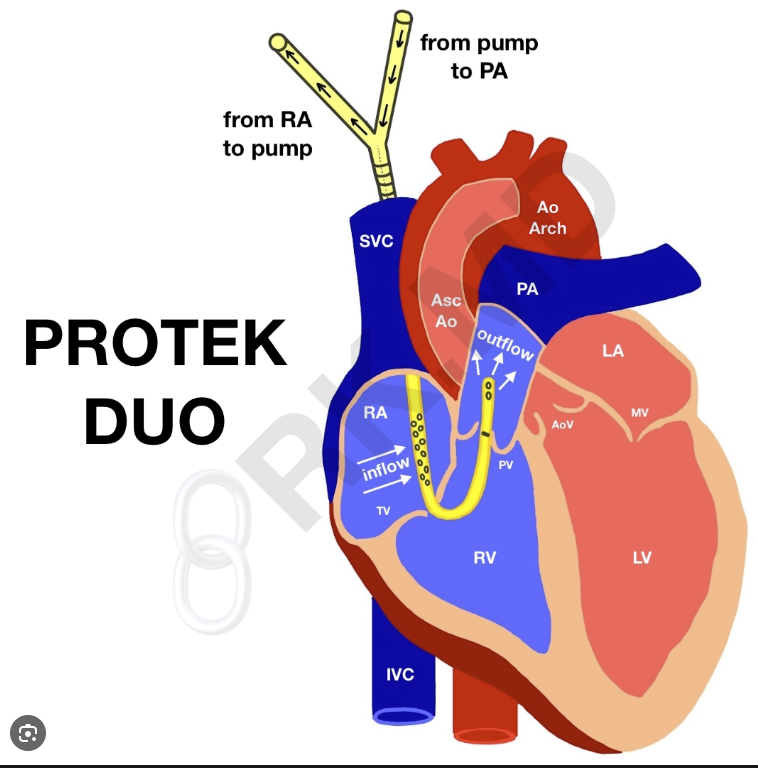
Protec Duo Cannula¶
This special VV ecmo is used when a patient is in isolated RV failure with oxygenation needs.
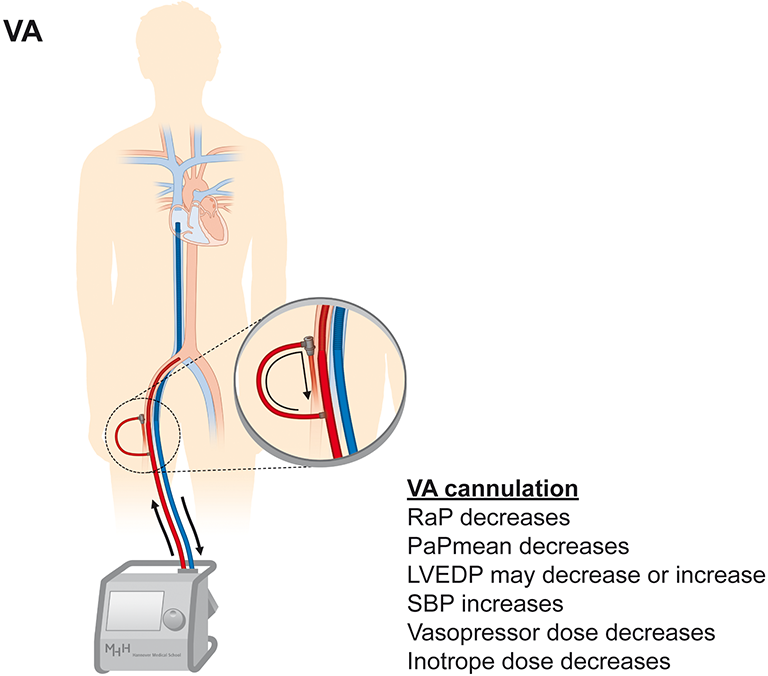
VA ECMO¶
Heart failure, cardiogenic shock, PE. Need to worry about North South syndrome. North being deoxygenated, and South being oxygenated. Also may lead to LV distension in poor outflow states consider VAV or impella or both.
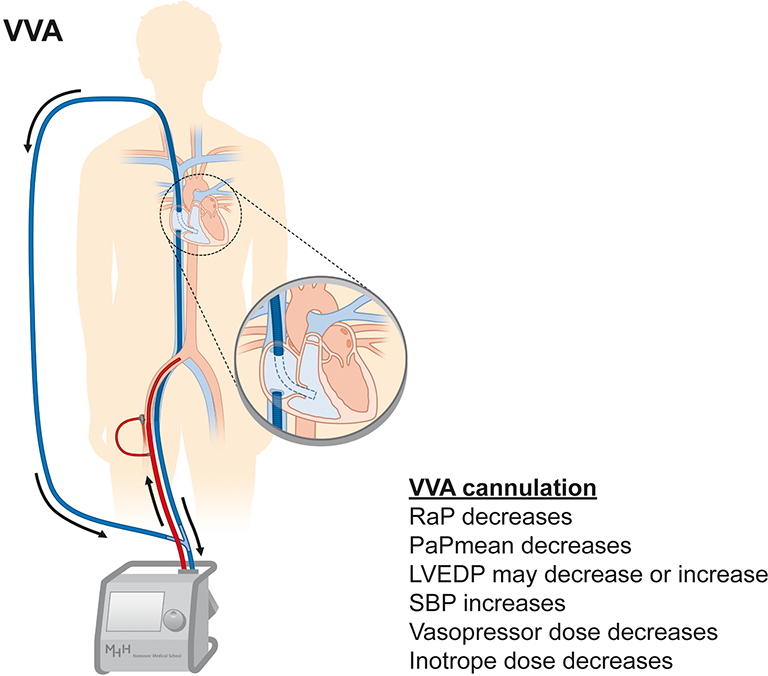
VVA ECMO¶
VA ecmo with increased drainage may help offload LV distension
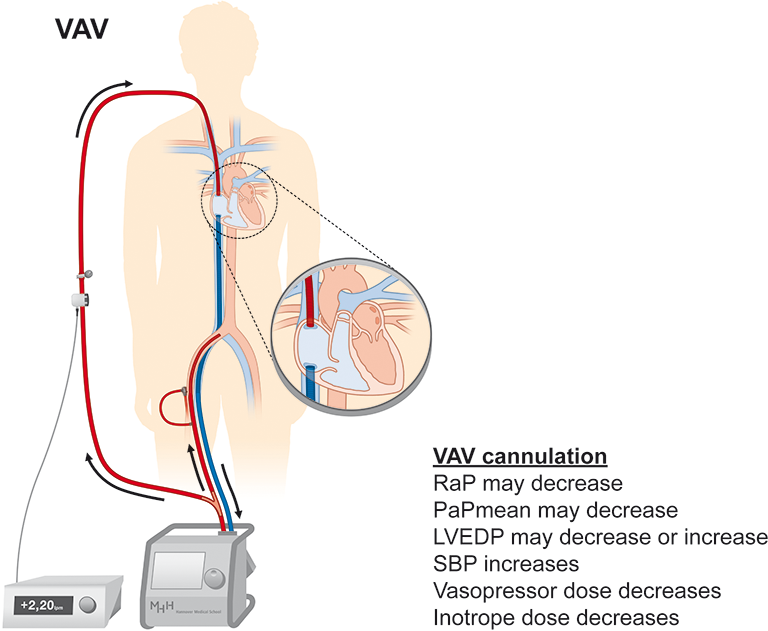
VAV ECMO¶
Combined VV and VA support. May need impella for LV distension
Impella Devices¶
J&J Med Tech formerly Abiomed Product Information
Device Overview¶
| Device | Access | Max Flow | Common Use |
|---|---|---|---|
| CP | Percutaneous | 3.7 L/min | Most common from cath lab |
| 5.5 | Surgical cutdown | 5.5 L/min | Longest duration (Can Ambulate) |
| RP Flex | IJ or Femoral Vein | 4 L/min | Full RV Unloading (Can Ambulate) |
TEE Positioning Verification¶
- Inlet (pigtail) in LV pointing toward apex
- Outlet in ascending aorta above aortic valve
- Straddling the aortic valve = malposition — reposition
- RP FLex should be beyond pulmonic valve with PA tracing
Aortic Insufficiency Complication¶
- Device crosses aortic valve — can worsen or unmask AI
- Signs: reduced flow despite good position, rising PCWP
- Large patients may exceed max flow capacity with significant AI
Suction Events¶
- Inlet against LV wall or septum
- Console alarm + sudden flow drop
- Fix: reduce speed briefly, give volume, reposition under TEE
Anticoagulation¶
- Purge solution: heparinized dextrose through device continuously
- Systemic heparin: target ACT 160-180 (lower than CPB)
- Do NOT use protamine if planning continued Impella support
Danger
Do NOT treat Impella-induced PVCs — they are mechanical. Do NOT reflexively volume load — Impella is already unloading LV. DO maintain MAP >65 — coronary perfusion depends on it.
ECMO with LV Impella ie ECPELLA¶
From the pdf:
VENOARTERIAL EXTRACORPOREAL MEMBRANE OXYGENATION (VA-ECMO) commonly is used to support patients with refractory cardiac arrest or cardiogenic shock mainly via percutaneous cannulation.4 This strategy may cause left ventricle (LV) distention that compromises myocardial recovery. Direct LV unloading provided by Impella was associated with lower mortality in patients with cardiogenic shock supported with VA-ECMO in a recent international multicenter study. The present paper has a specific purpose to provide a complete overview of this strategy, starting from a solid pathophysiologic approach. Then, the rationale for unloading the LV and the related available techniques is discussed. Finally, the combined configuration of VA-ECMO and Impella (ECPella) is fully treated, providing its significant clinical applications.
IABP Intra Aortic Balloon Pump¶
Mechanism: Diastolic augmentation (inflates in diastole to increase coronary perfusion), systolic unloading (deflates before systole to reduce afterload).
Timing modes: - ECG trigger — standard, uses R wave to time inflation - Pressure trigger — backup when ECG signal is poor
Weaning: 1:1 → 1:2 → 1:3 as patient stabilizes
Contraindications: Significant AR (worsens regurgitation), aortic dissection, severe peripheral vascular disease
Console: Watch augmentation waveform shape, trigger mode indicator, helium volume alarm
Removal: Surgeon removes while anesthesia manages