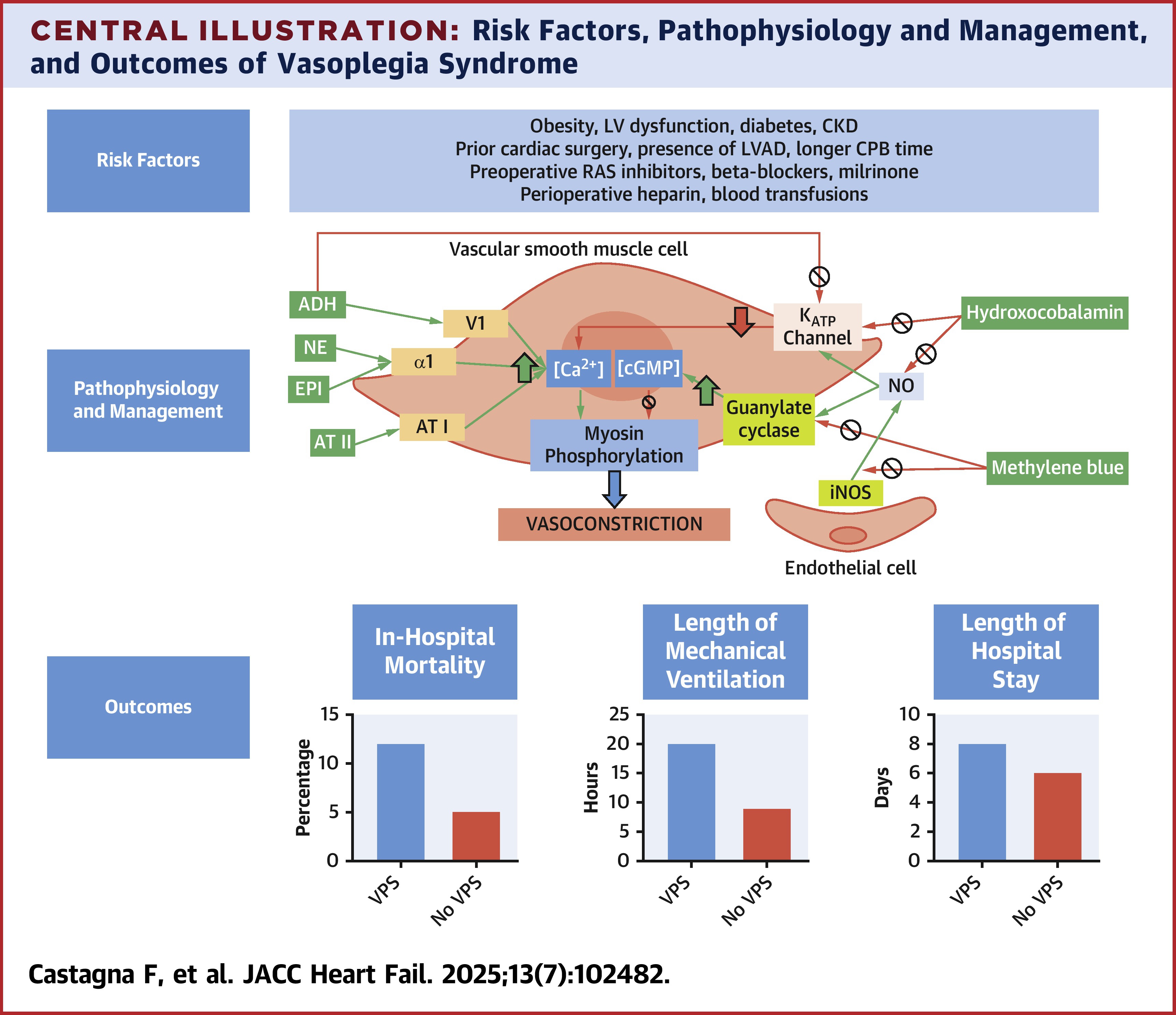
Vasoplegia¶
Vasoplegia is a type of distributive shock that follows cardiac surgery in up to 25% of cases. This leads to prolonged ICU stays, renal fialure, and increased mortality. Catecholamine resistant vasoplegia can be lethal with mortality rates approaching 25%. Vasoplegia can also exist in septic shock, end stage liver disease, and glucocorticoid deficiency.
Risk Factors¶
- Preoperative ACEi
- Higher comorbid disease burden
- Low preop EF
- Vasopressor support before and/or during CPB
- Warmer core temperature on CPB
- Long cross clamp time
Criteria¶
- MAP < 65 with an index of > 2.2
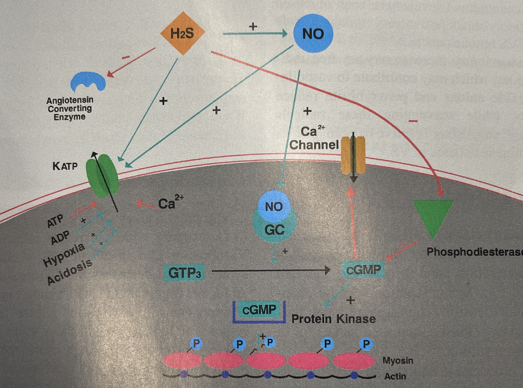
Physiology Simplified¶
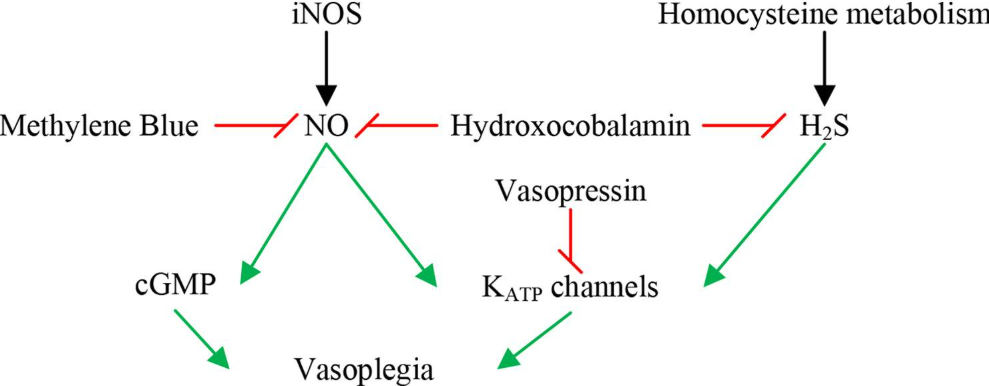
Specific Effect of H2S and NO¶
Treatment Goals¶
- Restore and Maintain MAP
- Vasopressors
- Inhibit vasodilatory mediators
- Methylene blue vs Hydroxocobalamin
- Goal directed fluid admin
- Improve Tissue Perfusion
- Fluids
- Inotropes
- Mechanical Support
- Prevent End Organ Damage
- Anemia treatment
- Assess renal, respiratory and cardiac function
- Identify and Treat Causes
- Immune suppression
- Steroids
- Histamine blockers
- Ascorbic acid/Thiamine
- Assess other factors
- Acidosis
- Hypovolemia
- Cardiogenic Shock
- Sepsis
- Medication/Transfusion Reaction
- Anaphylaxis
- Adrenal/Thyroid Crisis
Treatment Regimen¶
This is in order for the most part. I would recommend angiotensin II or vaso before epinephrine if the cardiac function is okay.
- Norepinephrine (0.02-0.5mcg/kg/min)
- Vasopressin (0.02-0.1un/min)
- Epinephrine (0.01-0.2mcg/kg/min)
- Angiotensin II (5-40ng/kg/min)
- Methylene Blue (1-2mg/kg bolus in 15min +/- 0.5-1mg/kg/hr infusion)
- Hydroxocobalamin (5g bolus over 15min can repeat x1)
- Hydrocortisone (50mg q6h or 100mg q8hr)
- Ascorbic acid (6g daily in divided doses per pharmacy)
- Thiamine (400 mg daily)
- Diphenhydramine (25-50mg q4-6h max 400mg in 24hr)
Comparison Between Methylene Blue and Hydroxocobalamin¶
A small sample size study showed no difference between the two treatment options when faced with vasoplegia status post cardiac bypass.
Summary¶